Aspergillosis in Raptors
6533 Views |

Aspergillosis in Raptors
By: Dr. Tong (Akkaraphat Butsurin, DVM)
Respiratory fungal diseases in raptors are most commonly caused by the Aspergillus species. Infection occurs through the inhalation of fungal spores present in the environment. Once inhaled, the spores colonize and multiply within the bird's respiratory system. The preferred sites for growth are warm and moist areas, particularly the air sacs.
Aspergillus is an opportunistic pathogen; it typically causes disease when the bird's immune system is compromised or weakened. Under normal conditions, a healthy immune system can effectively resist the fungus. However, stress plays a critical role as it triggers the release of cortisol, a hormone that suppresses the immune response. Common stressors include:
Relocation or changes in habitat.
Import and export processes.
Excessive or over-strenuous flight training.
Environmental changes.
Improper handling or aggressive medical restraint.
Pathogenesis
Once the fungus enters the respiratory tract, it triggers macrophages to perform phagocytosis (engulfing and destroying the spores). However, this process also triggers tissue damage by releasing free radicals and pro-inflammatory mediators, specifically Interleukin-1. This leads to severe inflammation of the respiratory tract, particularly air sacculitis.
Furthermore, the fungus secretes toxins:
Aflatoxin: Causes liver necrosis (death of liver cells).
Gliotoxin: (Specifically from Aspergillus fumigatus) further suppresses the immune system.
Clinical Signs
In the early stages, clinical signs may be absent. Respiratory symptoms are the most common and prominent indicators, including:
Dyspnea (difficulty breathing), open-mouth breathing, or increased abdominal effort.
Tail bobbing.
Voice changes (hoarseness or loss of voice).
Exercise intolerance (unable to endure flight training).
Non-specific signs: Weakness, drooping wings, or increased green urates/feces.
Note: Respiratory symptoms often mimic other diseases. Accurate differential diagnosis is required to rule out:
Psittacosis (Chlamydiosis).
Bacterial respiratory infections.
Foreign body aspiration.
Mycobacterium spp. infections.
Respiratory neoplasia (tumors/cancer).
Risk Factors: Increased atmospheric humidity combined with the bird's internal body temperature provides an ideal environment for fungal growth. Therefore, birds imported from abroad are at a higher risk of developing the disease in Thailand's climate.
Diagnosis
Clinical signs are often non-specific. Patient history frequently reveals unhygienic living conditions or poor environments. Chronic weakness, weight loss, or voice changes are significant red flags. Diagnostic tools include:
Hematology: Characterized by marked leukocytosis, specifically severe heterophilia with a left shift, monocytosis, and lymphopenia. Chronic cases may show non-regenerative anemia.
Biochemistry: Low albumin-to-globulin ratio, and elevated AST and bile acids if liver involvement is present.
Serology (Indirect ELISA): Highly useful for diagnosis and monitoring disease progression or treatment response. Antibodies can be detected within one week post-infection, often before clinical signs appear, allowing for more effective early treatment.
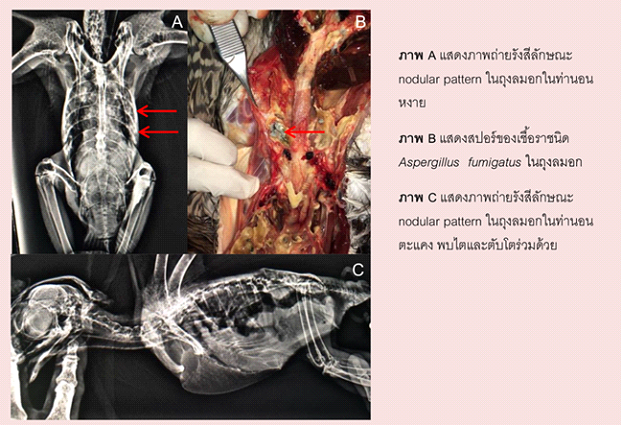
Radiography: May show a parabronchial or nodular pattern, asymmetrical air sacs, or cloudiness/thickening of the air sacs due to fungal growth and inflammation. Lesions are commonly found in the cranial abdominal air sacs and lungs. Hepatomegaly (enlarged liver) or renomegaly (enlarged kidneys) may be visible if systemic spread has occurred. Generally, if radiographic changes are visible, the prognosis is guarded as the disease is likely advanced.
Treatment
Treatment is complex because antifungal drugs often have difficulty reaching the fungal lesions. For granulomatous lesions, surgical debridement (trimming away the growth) is the best option, though it is technically difficult and carries a high surgical risk. A combination of nebulization and systemic therapy is often recommended.
Pharmacology
Itraconazole: Specific for Aspergillus. Dosage: 5 mg/kg PO BID (twice daily) or 10–15 mg/kg PO SID (once daily). Dosage depends on the bird's response, as high doses can cause depression or anorexia. It is hepatotoxic, with sensitivity varying by species. Absorption is enhanced when administered with fats.
Amphotericin B: Used for severe infections. It has poor oral absorption and is irritating if given IM or SC. In severe respiratory cases, it can be given IV at 1.5 mg/kg TID. It is relatively non-toxic to the kidneys in birds even with long-term use. It can also be applied topically to air sacs at 0.5 mg/ml during endoscopy.
Flucytosine: 20–60 mg/kg PO BID, often used in combination with Amphotericin B for long-term treatment (6 months or more).
Fluconazole: Highly water-soluble and quickly absorbed. It can cross the blood-brain barrier (CSF), enter brain tissue, ocular fluid, and sputum. It is the drug of choice for CNS involvement. Dosage: 15 mg/kg PO BID.
Ketoconazole: 20–30 mg/kg PO BID for 2–6 weeks. Can be used in combination with other antifungals but does not penetrate the CSF or ocular fluid.
Polymeric Fluoropyrimidine (F10): Used via nebulization for the bird and for environmental disinfection to reduce spore load.
: What Exactly Is It?")


